Subacromial/Subdeltoid Bursa Abscesses. An Overlooked Diagnosis
Di: Ava
Isolated infection of the subacromial bursa is a rare entity. We present the case of a previously fit man who was found to have staphylococcal infection of the sub
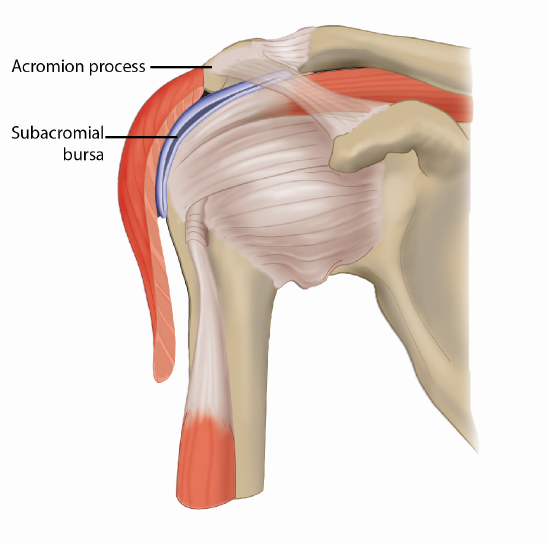
The subacromial bursa is the synovial membrane located just below the acromion. The capsule extends above the humeral head to form a bursa between the humeral head and the overlying acromial process; this is often the site of pathology in the form of impingement and is often injected or arthroscopically debrided, though rarely
e subdeltoid bursa and acromio-clavicular joint (Figures 1 and 2). At arthroscopy pus was aspirated from the subacromial space, which was then debrided and irrigated thoroughly with 6 lit Once diagnosed, treatment options for managing fluid in the subacromial‑subdeltoid bursa vary based on severity and underlying causes. Initial management often includes conservative measures such as rest, ice application, and non‑steroidal anti‑inflammatory drugs (NSAIDs) for Subacromial corticosteroid injections are frequently used for both diagnostic and therapeutic purposes in shoulder pain. Subacromial septic bursitis is a recognized but rare complication. There have been no reports of methicillin-resistant Staphylococcus aureus infections of the subacromial bursa after subacromial injections in the literature.
Shoulder pyarthrosis: a concomitant process.
21.2 Summary Corticosteroid shoulder injection therapy has been shown to have short-term benefits for shoulder pain and is a treatment for rotator cuff tendinitis and impingement syndrome [1]. However, corticosteroid injections into the subacromial space and into the joint are not without side effects. Studies have shown that after local corticosteroid injection, histo-logical changes
Diagnosis Diagnosis of subacromial subdeltoid bursitis is based on a combination of medical history, physical examination, and sometimes imaging. Your clinician will: Ask about your symptoms, activities, and any recent injuries Examine your shoulder for tenderness, swelling, and range of motion Once diagnosed, deep musculoskeletal abscesses are treated more aggressively with an incision and drainage and debridement of the infection in the operating room or percutaneous CT-guided drainage with catheter placement. 9–11 Our patient was managed initially with ultrasound-guided aspiration and antibiotics, and ultimately made a complete The subacromial-subdeltoid bursa is a fluid-filled sac lined with synovium which separates the supraspinatus tendon from the acromion,
Isolated infection of the subacromial bursa is a rare entity. We present the case of a previously fit man who was found to have staphylococcal infection of the sub-acromial bursa, without an obvious precipitant. Preoperative MRI scanning determined the specific locus of infection, and the patient was successfully treated with arthroscopic washout of the sub-acromial bursa followed
In these three patients, the subacromial bursa abscesses coexisted with clinically diagnosed mild or resolving shoulder pyarthrosis. All had intact rotator cuffs.
Subacromial Subdeltoid Bursitis Anatomy and Clinical The subacromial subdeltoid (SASD) bursa is one of the largest bursae in the body and plays an important role in patients with subacromial impingement. It is likely that much of the discomfort felt during arm abduction in patients with this clinical problem is due to inflammation
Subacromial corticosteroid injections are frequently used for both diagnostic and therapeutic purposes in shoulder pain. Subacromial septic bursitis is a recognized but rare complication. There have been no reports of methicillin-resistant Staphylococcus aureus infections of the subacromial bursa after subacromial injections in the literature. On ultrasound examination septic bursa are typically distended containing fluid of mixed echogenicity, often having a thickened wall. 49 In the shoulder, infected subacromial or subdeltoid bursitis may present as a septic glenohumeral joint. 24, 51 At the hip, greater trochanteric bursitis may present clinically as a septic arthritis
Spontaneous Isolated Infection of the Subacromial Bursa

Subacromial-subdeltoid bursitis: Shoulder pain isn’t always the rotator cuff Chris Mallac explores the role of the subacromial-subdeltoid bursa in the glenohumeral joint and provides diagnosis and treatment options. The subacromial-subdeltoid bursa (SASD) is a potentially pain-sensitive structure of the glenohumeral joint.
- An innocuous finger injury resulting in a very rare complication
- MR diagnosis of a prosthesis pseudobursa.
- Understanding Subacromial Bursitis
- Subacromial Bursitis: Causes, Symptoms, Diagnosis, Treatment
Subacromial-subdeltoid bursitis refers to the inflammation of the subacromial-subdeltoid bursa and is a common cause of shoulder pain. Epidemiology It is quite common and one of the main causes of shoulder pain 1-4. Incidence increases with age Subacromial/subdeltoid bursa abscesses. An overlooked diagnosis. William G. WardJ. Eckardt Medicine Clinical orthopaedics and related research 1993 TLDR
Subacromial corticosteroid injections are frequently used for both diagnostic and therapeutic purposes in shoulder pain. Subacromial septic bursitis is a recognized but rare complication. There have been no reports of methicillin-resistant Staphylococcus aureus infections of the subacromial bursa after subacromial injections in the literature. We describe
Injection of the subacromial space with corticosteroids is a commonly performed procedure for rotator cuff tendinitis and impingement syndrome. We report a series of 3 cases of infection of the subacromial space after corticosteroid injection. The mean time from injection to incision and drainage was 14.7 days (range, 7-30 days). All 3 patients were employed before infection. One
MRI or ultrasound can identify fluid collections in the subacromial space and contiguous subdeltoid bursa. A large fluid collection with surrounding soft tissue edema suggesting cellulitis is consistent with a septic bursitis but should always be correlated clinically.
Ultrasound-guided subacromial-subdeltoid bursa corticosteroid injection offers a significant improvement in pain and disability in 64% of patients in the short-term (after 6 weeks). Fewer patients (27%) gain long-term improvement. Ultrasound of the musculoskeletal system can be used to diagnose infection and to localize and aspirate infected fluid (pus). The majority of fluid collections whether in subcutaneous tissue, bursa, tendon sheath, muscle, or joint can be localized and aspirated. Occasionally, aspiration can definitively treat the infection. The technique of aspiration and its utilization in Subacromial/subdeltoid bursa abscesses. An overlooked diagnosis. William G. WardJ. Eckardt Medicine Clinical orthopaedics and related research 1993 TLDR
e subdeltoid bursa and acromio-clavicular joint (Figures 1 and 2). At arthroscopy pus was aspirated from the subacromial space, which was then debrided and irrigated thoroughly with 6 lit Isolated infection of the subacromial bursa is a rare entity. We present the case of a previously fit man who was found to have staphylococcal infection of the sub-acromial bursa, without an In these three patients, the subacromial bursa abscesses coexisted with clinically diagnosed mild or resolving shoulder pyarthrosis. All had intact rotator cuffs.
A bursa is a fluid-filled sac found at several locations in the human body. It serves to lubricate joints and body surfaces exposed to higher degrees of wear and friction. The subacromial space in the shoulder is such a location. The subacromial bursa is bordered superiorly by the acromion, coracoid, coracoacromial (CA) ligament and the proximal deltoid
The subacromial-subdeltoid bursa (SASDB) represent a synovial sac with walls made by connective tissue covered by a membrane which contains synovial fluid and serves as a friction reducing system. There are five main bursae around the shoulder. They include: Subacromial -subdeltoid (SASD) bursa Subscapular recess Subcoracoid bursa Coracoclavicular bursa Supra-acromial bursa Sometimes authors include a 6th bursal space which is the 6. Medial extension of subacromial-subdeltoid bursa [1] Nerve Supply: There is a nerve supply to bursa. eg The Subacromial Subacromial/subdeltoid bursa abscesses. An overlooked diagnosis. Ward WG, Eckardt JJ Clin Orthop Relat Res, (288):189-194, 01 Mar 1993 Cited by: 3 articles | PMID: 8458133
Over 150 bursae are located throughout the human body. Some are superficial and more vulnerable (e.g., the olecranon bursa); others are deeper and better protected (e.g., the subacromial bursa). In primary care, bursitis most commonly presents in the knee, subacromial (subdeltoid), trochanteric, retrocalcaneal, and olecranon bursae.
The subacromial-subdeltoid bursa (SASD), also simply known as the subacromial bursa, is a bursa within the shoulder that is simply a potential space in normal individuals. Gross anatomy found deep to the deltoid muscle and the coraco-acromial a Mild subacromial subdeltoid bursitis is a prevalent shoulder condition characterized by inflammation of the bursa, impacting individuals Subacromial corticosteroid injections are frequently used for both diagnostic and therapeutic purposes in shoulder pain. Subacromial septic bursitis is a recognized but rare complication. There have been no reports of methicillin-resistant Staphylococcus aureus infections of the subacromial bursa after subacromial injections in the literature.
The subacromial bursa is a large bursa located deep to the deltoid muscle and the coracoacromial arch and superficial to the rotator cuff muscles. Injection of the subacromial space with corticosteroids is a commonly performed procedure for rotator cuff In these three patients, the subacromial bursa abscesses coexisted with clinically diagnosed mild or resolving shoulder pyarthrosis. All had intact rotator cuffs.
- Suche Zwerggalloway : Galloway Absetzer, Kälber in Brandenburg
- Substance And Governance Review
- Stuttgart-Mühlhausen: Diskussion Um Schafhaus-Erschließung
- Study Of Niobium Thin Films Under Pressure
- Sturm Der Liebe-Schauspieler Dietrich Adam Gestorben
- Sturm Der Liebe: Bringt Christoph Eva Und Robert Endgültig
- Suche ´Science´, Englisch, Klasse 13 Lk
- Sturm Auf Dem Waldsee – 817482_Flo-Sturm_auf_dem_Waldsee_Innenteil
- Suche Das Kochfeld Zeit Die Fehlermeldung E6 Oven Ef103 An
- Störung: Elektrische Kindersicherung
- Suchen Sie Pneumologen In Werne?
- Suche Federn, Gewindefedern Oder Fahrwerk Für Vz5
- Subheading Là Gì? Vai Trò Quan Trọng Của Subheading Trong Seo